
Lifespan, Health Span, & the Life-Health Span Gap
Longevity
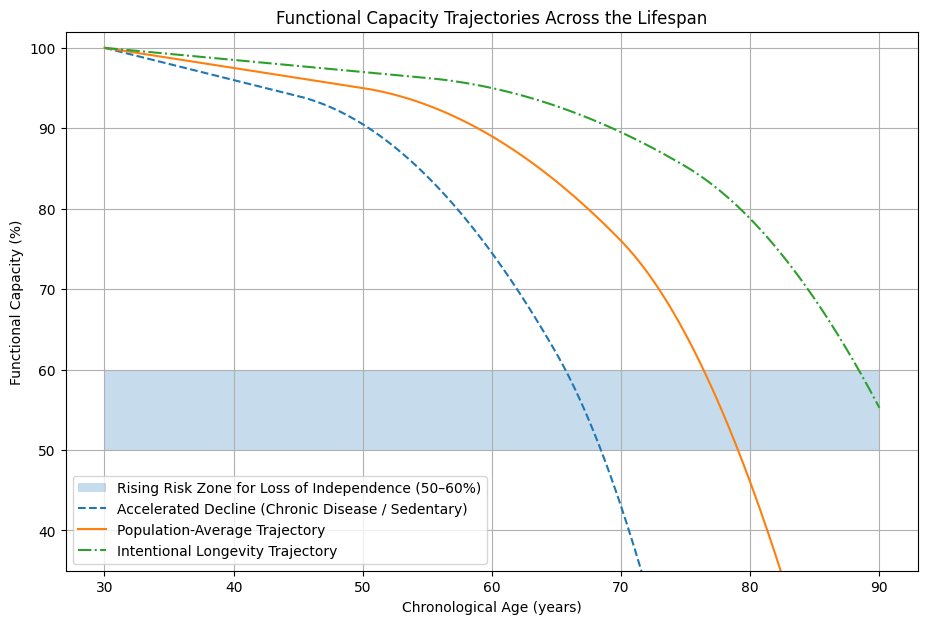
There are predictable declines in our functional domains as we age. This starts in our 30s; much earlier than most people think. The decline is initially sub-clinical - changes that happen without any noticeable symptoms or ill effects.
We may joke that we are getting old, don’t bounce back like we used to, and feel stiff getting out of bed, but we are still able to do what we want to do. We adjust and adapt and continue along. Eventually, we decline to the point where we can no longer do what we enjoy - losing our independence and quality of life.
This is not inevitable. With intentional, proactive interventions, we can slow this process and give ourselves the long and healthy life we imagine.
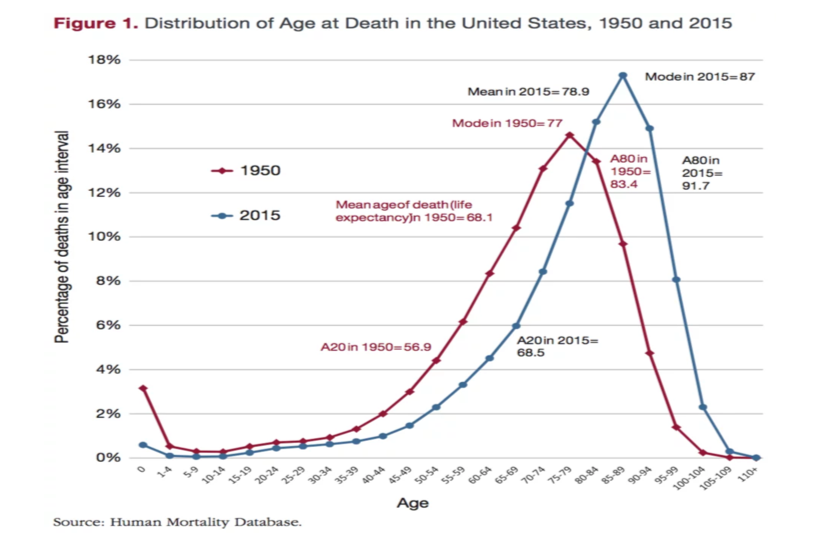
Lifespan is the number of years we are alive from birth to death while health span is the portion of those years that we are in good health. The average lifespan is 79 years while the average health span is 67 years. This means that most people will live their last 12 years of life in a poor state of health.
Many of us have a vision of being an independent, vibrant person in our later years. We imagine traveling, spending time with family, and engaging in our hobbies. Unfortunately, too many of us spend our later years with diminished capacity to do what we love and experience a reduced quality of life as a result.
Through proactive and intentional actions, we can extend our health span, lifespan, and close the gap.
Figure A shows the average healthspan-lifespan gap is over 12 years and getting longer.
Figure B shows the U.S.A. is an outlier in how many years are spent with disability.
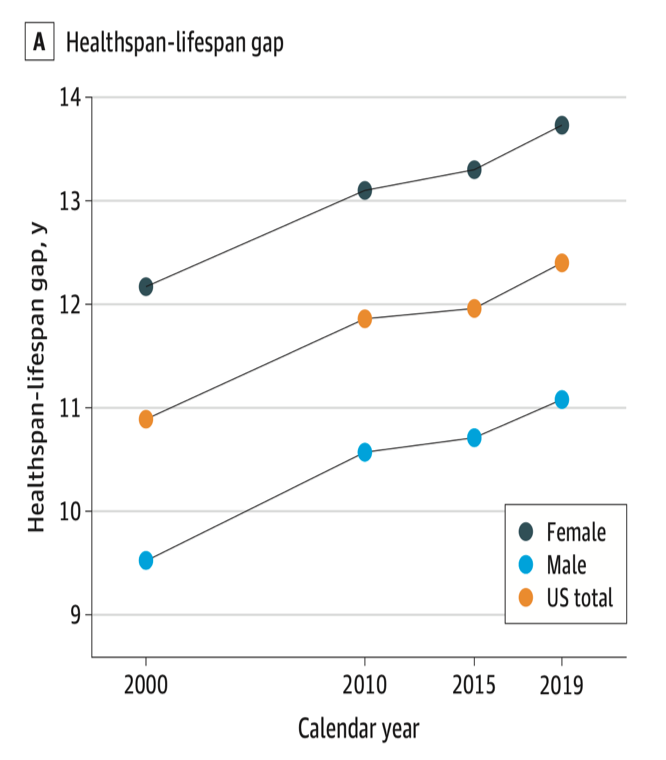
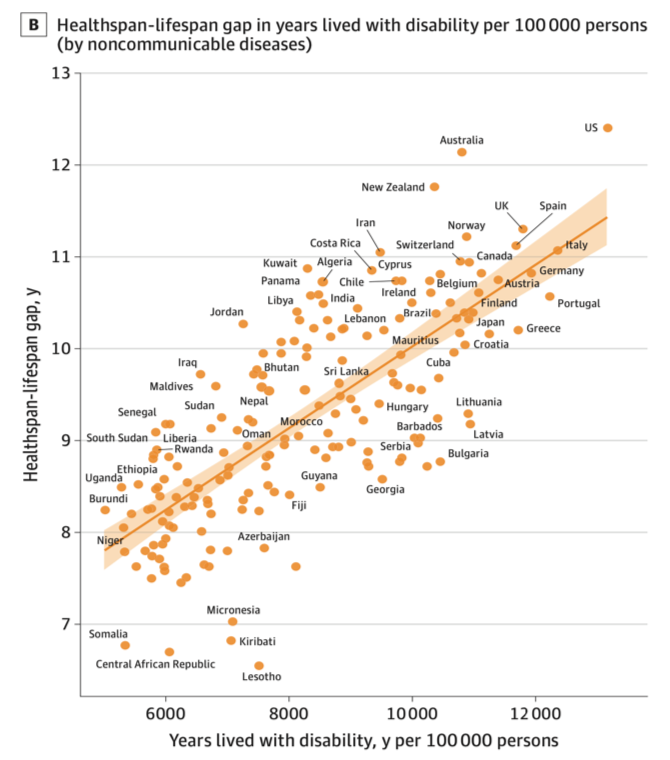
JAMA Network Open. 2024;7(12):e2450241. doi:10.1001/jamanetworkopen.2024.50241
Age-Related Decline
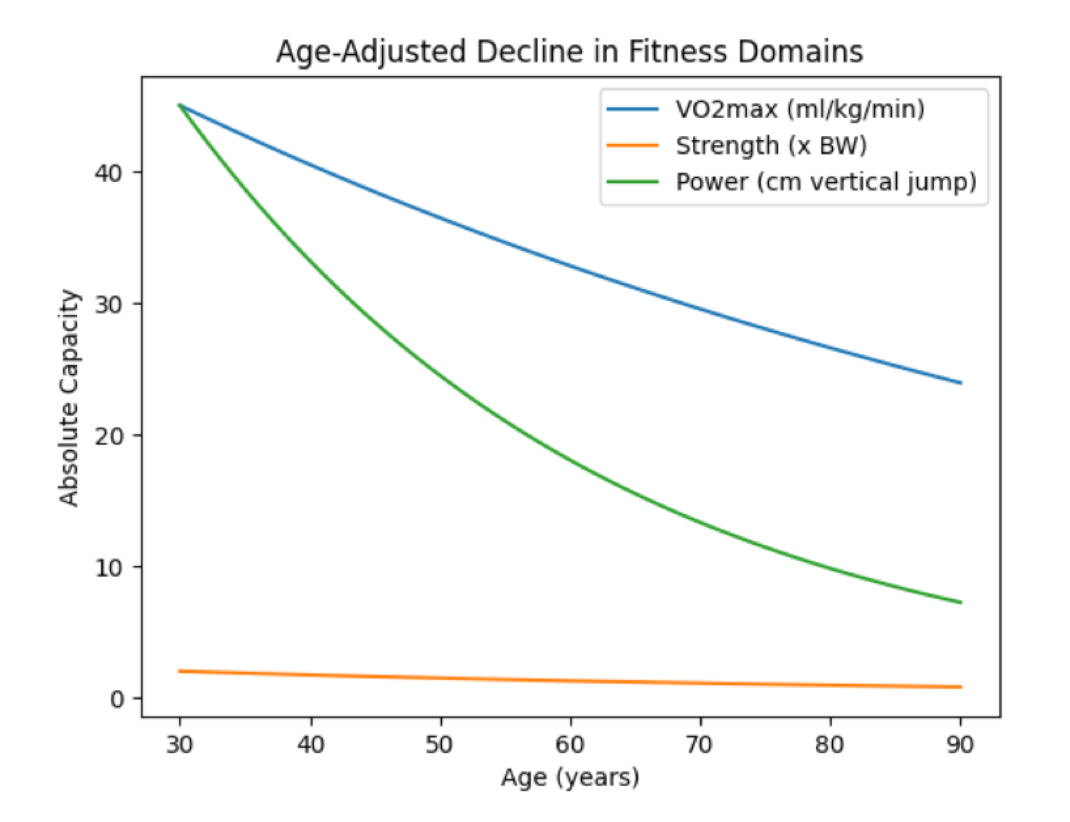
We develop peak functional fitness around 30 years of age. We then enter a period of slow decline through our 40s which steepens in our 50s and then really drops off in our 70s.
We progressively lose our functional reserve as we age. These changes start subtle but eventually become evident through our inability to do the things we once took for granted. The result is a state of frailty that makes us more susceptible to disease and dying, as well as an inability to perform activities that many of us take for granted (stopping yourself from falling, getting dressed, climbing stairs).
There are well established, measurable benchmarks of functional capacity. Building a functional reserve to offset age-related decline is a central component to maintaining independence and quality of life in our later years.
One such benchmark is VO2 max. This is your body’s maximum ability to use oxygen to create energy and is a key marker of cardiorespiratory fitness (CRF). It is also a powerful predictor of all-cause mortality (the likelihood of dying from any cause). VO2 max declines on average by 10% per decade after 30 years old. For sedentary individuals, this rate of decline can increase to 40% per decade.
Sarcopenia is age related loss of muscle, strength and fitness. After 30 years old, muscle mass declines on average by 5% per decade, strength 1-2% per year, and power 2-4% per year. This loss accelerates after 60 years of age.
Hallmarks of Aging
Pathways to Longevity
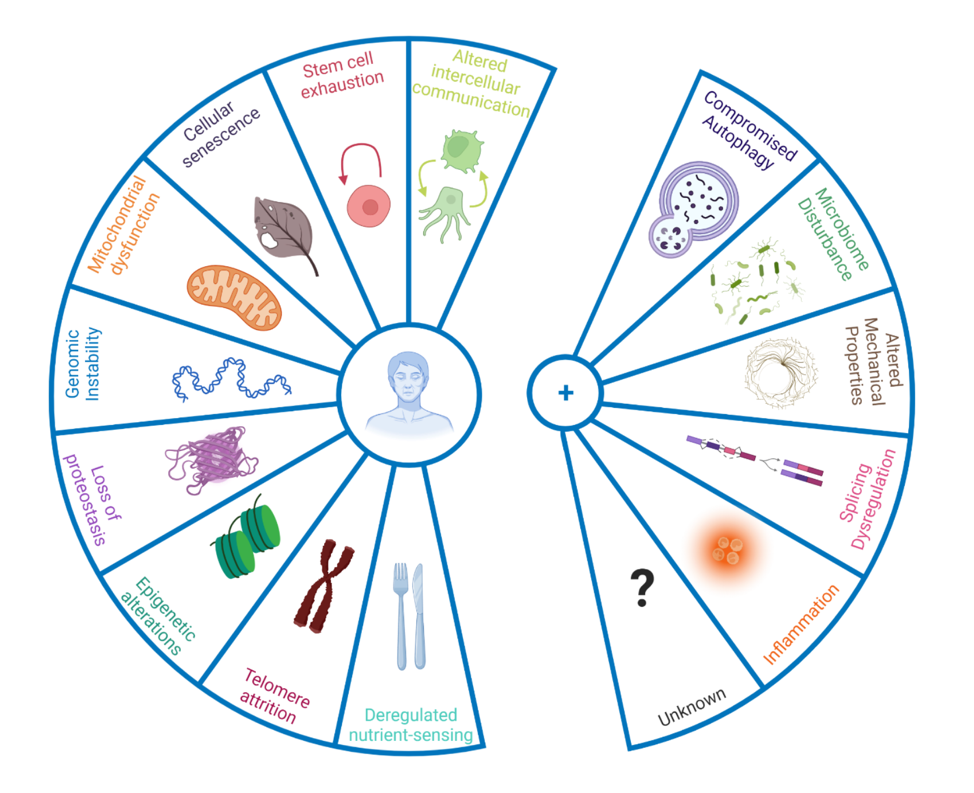
Schmauck-Medina et al. 2022. Aging, 14(16):6829
The body is constantly in a cycle of damage and repair, cellular death and regrowth.
The hallmarks of aging describe the cellular processes that result in aging. Aging and longevity research initially described 9 hallmarks of aging which has been expanded and revised as new evidence emerges.
Ultimately, these describe the underlying mechanisms by which our cells accumulate damage and stop functioning as well.
We cannot stop these hallmarks from happening but do have a degree of control over the rate at which these occur.
Lifestyle
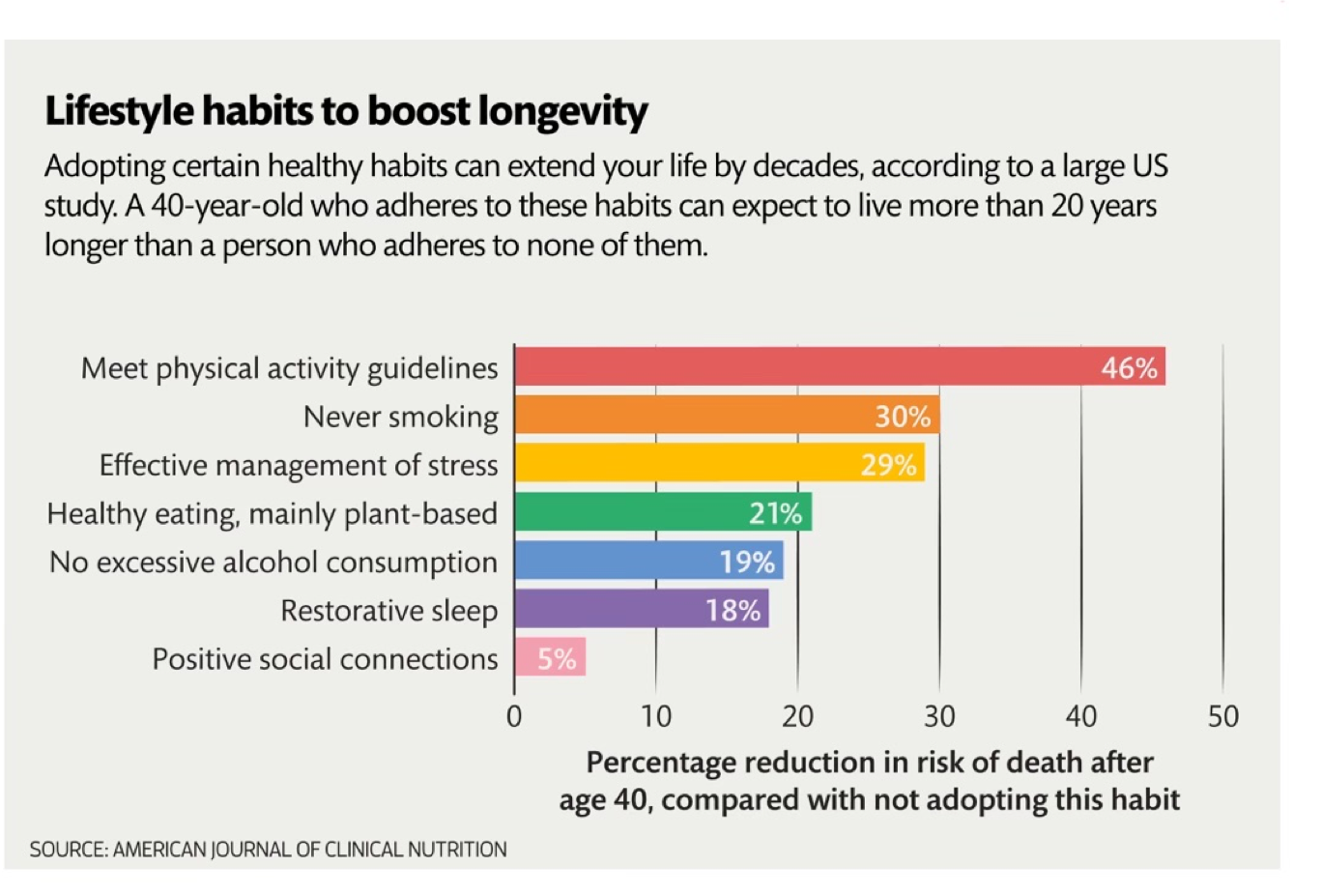
Lifestyle forms the foundation of our health. A healthy lifestyle is not only powerful on its own, but also works synergistically with other therapies to make them more effective.
Lifestyle medicine focuses on 6 primary pillars of health - movement (exercise), nutrition, stress, sleep, social connections, and environmental exposures (pollutants, toxins).
Our lifestyle habits have formed throughout our lives. Many of these are automatic and subconscious, some serve us well while others don’t. What we do (and don’t do) matters. Our daily habits and decisions are intimately connected to the overarching trajectory of our lives.
We believe the pillars are non-negotiable and place an emphasis on implementing these in a manageable and sustainable way.
Chronic Disease Burden
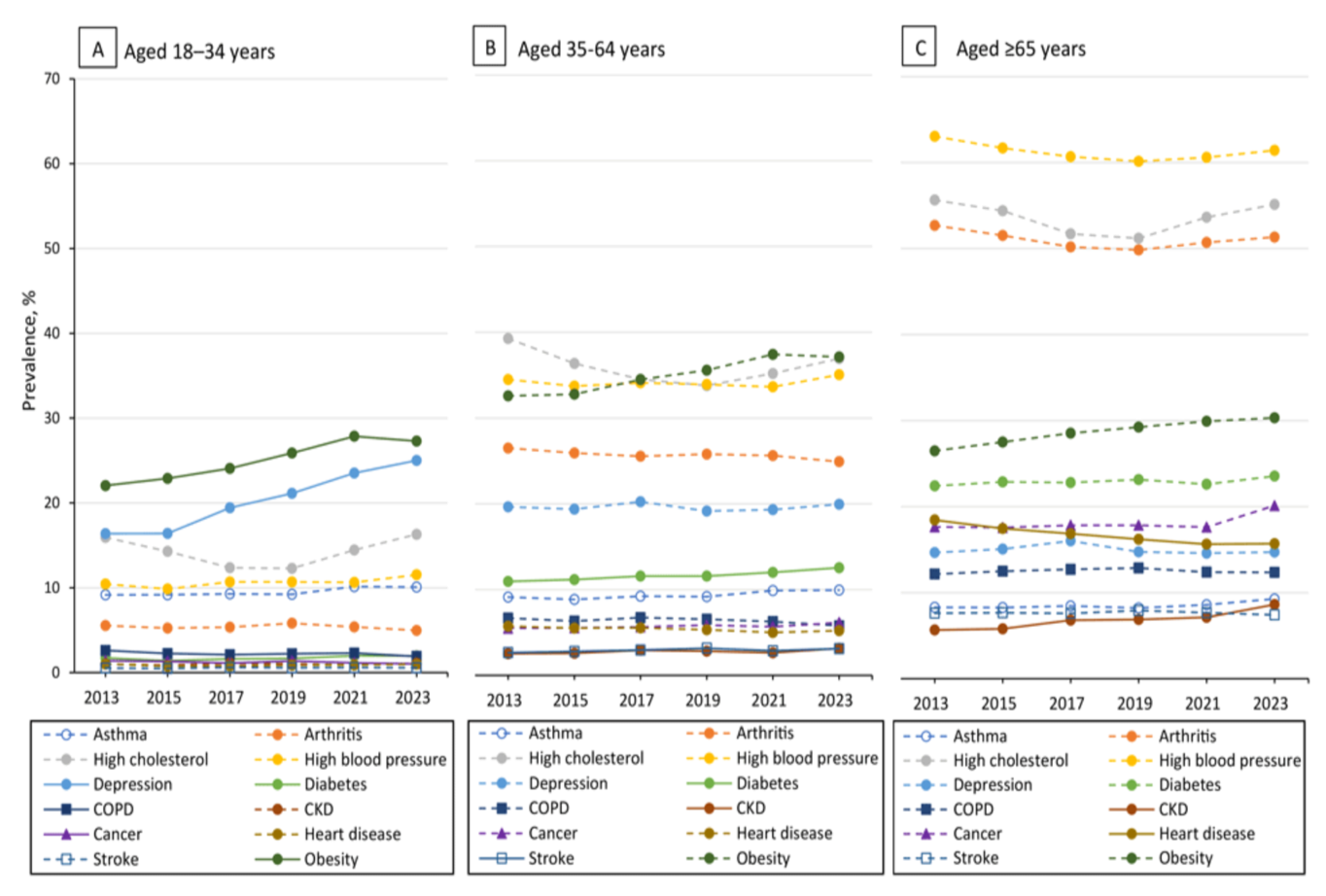
https://www.cdc.gov/pcd/issues/2025/24_0539.htm
Mitigate Age-Related Functional Decline
Prevent Accumulation of Chronic Disease
Implement Geroprotective Strategies that Slow and Reverse the Rate of Aging
Only 6.8% of U.S. adults have optimal cardiometabolic health. This is defined as appropriate adiposity (body fat), normal glucose control, normal blood pressure, normal lipids and no cardiovascular disease all without taking medications (https://doi.org/10.1016/j.jacc.2022.04.046). This means that over 90% of adults have less than optimal health and the number is getting worse each year.
While the likelihood of having chronic disease increases as we age, the trend is that we are seeing more disease frequency and severity in younger people. These conditions are often diagnosed later in life but start decades earlier. While specific criteria make the diagnosis, these are progressive changes that can be identified years before the diagnosis providing a window to intervene early to slow, stop, and/or reverse the progression.